 English
English Español de México
Español de México Português
Português Français
FrançaisMost citations used are taken from the NLM data base and are in the public domain.
MTHFR MUTATIONS AND FAULTY EGG DIVISION
In 1998 I was collecting family history data on the maternal line in children with Down syndrome. I was extremely curious about the apparent high number of identical twins in these families. Jill James, research scientist and folate expert, and I noticed that there was also a higher than average occurrence of Spina Bifida in the maternal line. My first thought, after looking at the compiled information, was that somehow DS pregnancies were related to MTHFR mutations. This is the same gene mutation responsible for Spina Bifida. Jill applied for funding to test this theory but as anticipated, obtaining it was difficult based solely on these data.
Fortunately, I located the results of a five year trial done in New South Wales that followed birth defects after fortifying foods with folic acid. And there it was in black and white. This study contained a table listing several birth defects, including DS, and the number of live births both prior to and after the addition of folate. Down syndrome and Spina Bifida fell by identical margins. This suppiorting information enabled us to obtain funding and a year later the results of our study were published. The incidence of MTHFR mutations in mothers of children with Down syndrome was scientifically and statistically significant. Since this, the very first work connecting DS to an actual “cause” the study has been repeated over thirty times by researchers world wide. It is clear that a maternal folate deficiency interferes with chromosome segregation during first phase meiosis causing the equal division of the egg to fail. The underutilized egg containing 24 chromosomes may be viable while the egg with 22 chromosomes is not.
Recent testing of single nucleotide polymorphisms have identified two genes with mutations that may also produce the same effect, the inability of the human body to properly metabolize folate. These are MTRR and CBS mutations.
What is MTHFR
MTHFR is a gene mapped to chromosome 1 (1p36.3). It encodes for an enzyme, 5,10-methylenetetrahydrofolate reductase. This enzyme is important in the conversion of folic acid into its active form. Until this conversion takes place the human body cannot utilize folic acid. It is also important in the process of converting homocysteine into methionine but, for this discussion, we will focus is on folate.
Folate is actually Vitamin B9. It is found in its inactive form in certain fruits and vegetables, used to fortify foods and is included in most multi vitamin supplements. Without it, DNA cannot be created or repaired and cells cannot divide. This function is targeted by many forms of chemotherapy. For instance, the drug Methotrexate, inhibits an enzyme in folate metabolism called DHFR – Dihydrofolate reductase. Inhibition of DHFR stops the folate cycle. Rapidly dividing cells such as cancer and hair cells are unable to reproduce After Methotrexate, a ‘rescue’ must be performed by providing the patient with folate or slower dividing cells would also die. Without sufficient folate, the human egg fails to properly divide during first phase meiosis and a number of anomalies can result, including the addition to an egg of an extra chromosome. This is known as nondisjunction.
It is important that you understand two things. 1) it is not your fault that your baby was born with DS as you likely had no idea you suffer from this mutation and 2) it is not difficult to overcome it. The addition of a sufficient form of active folate, methyltetrahydrofolate and B12 will usually insure normal chromosome segregation barring anything that may interfere with absorption or the cycle itself. A natural catachin found in green and black tea and apples, epigallocatechin-3-gallate (EGCG) inhibits DHFR in dose dependent amounts much like Methotrexate and should be avoided when trying to conceive. Alcohol and even stress can interfere with folate absorption as can a lack of beneficial gut bacteria. This bacteria is destroyed by antibiotics, so the use of them while trying to conceive may be also an issue, though this is unproven.
Regardless of what you may have read elsewhere untreated hypothyroidism does NOT cause Down syndrome. It is related to a number of problems, pre-term labor, placental abruption, low birth weight, learning and developmental delay, but it does not interfere with egg division. However Hashimotos Thyroiditis is associated with MTHFR mutations so it is possible for a woman who gives birth to a child with DS to also have Hashimotos but it is not in anyway connected to faulty egg segregation. Too much folic acid does NOT cause Down syndrome unless the folate is not metabolized and becomes trapped. When that occurs the result is a folate deficiency.
While the majority of mothers of children with Down syndrome have one or more MTHFR mutations, women without them also give birth to infants with chromosome abnormalities. This is likely the result of a severe folate deficiency at the moment of first phase meiosis unassociated with gene mutation.
In rare cases, Down syndrome is inherited. This usually occurs when an egg already contains an additional section of the critical region prior to meiosis. The Down syndrome critical region (DSCR) is a portion of the p leg of the maternal half of the chromosome. This usually is attached to another chromosome. Because the entire portion of the DSCR is present, the child will be born with Down syndrome despite the absence of the complete chromosome. This is referred to as translocation.
A third form of DS is mosaicism. In mosaic Down syndrome, the child has two cell lines. One contains 46 chromosomes while the other contains 47. Mosaicism occurs when nondisjunction happens after fertilization, during mitotic cell division. Children with mosaicism can be only mildly affected even if the level of mosaic cells exceeds those of normal cells. They may also be as affected as non mosaic children. The level of function in all three forms of Down syndrome varies widely.
Why don’t all of my children have DS?
MTHFR mutations are not difficult to overcome, Despite the presence of a mutation, you may have sufficient folate available at the nano second of first phase meiosis for normal cell division. Another possibility is that although a fertilized egg containing 47 chromosomes can be viable, the incidence of viability is low. The fact that a child with Down syndrome actually comes to term is itself miraculous when you couple low egg viability with a higher than 80% loss in the first weeks of pregnancy.
Your chances of a second, full term DS pregnancy are low. However many siblings of children with Down syndrome have learning disabilities, ADHD, autism, autoimmune disorders and other disorders. It is unknown whether all are associated with an MTHFR mutation but some they may be. An MTHFR mutation should not be ignored as it results in numerous diseases, including Alzheimer’s disease and cardiovascular problems. Taking the appropriate measures to help your body overcome MTHFR mutations is the smart thing to do whether or not you are considering having more children.
Why is it rare for the father with an MTHFR mutation to contribute the extra chromosome?
Unlike the human egg, sperm are mobile. Though thousands of sperm race to compete to fertilize a ripened egg, only one succeeds. Once an egg is penetrated, the outer layer of the egg immediately repels and prevents other sperm from entering.
While men certainly can carry one or more polymorphisms that interfere with chromosome segregation at the stage of sperm meiosis, only rarely is trisomic sperm successful in fertilization. There are several theories, all of them possible. 1) as with a trisomic egg, few trisomic sperm survive meiosis. 2) Extra genetic material may effect the mobility of sperm, making it more unlikely that a trisomic sperm will be first to fertilize the egg. 3) a trisomic sperm may not be fertile.
Regardless of whether it is egg or sperm, no parent is ever at fault. Parents have no control over the mutations they inherit. Since these are silent mutations, where symptoms to the mother or father are often present but unrecognized, they simply go undiagnosed.
If you have one of these mutations, there are simple ways to reduce your chances of chromosome segregation errors.
1) Give yourself three full cycles prior to attempting conception.
2) Start immediately on a multi vitamin supplement containing Methylcobalamin (methyl B12), Methyltetrahydrofolate (active folate) and Betaine (a substance present in the folate cycle. I suggest Nutrivene Full Spectrum or Thorne Methyl Guard.
3) Avoid anything containing EGCG such as green tea, black tea and apples.
4) Do not drink any alcohol.
5) Avoid excess stress.
Be comfortable with the cards life has played for you. Down syndrome is not a tragedy, it can be a blessing. With TNI your baby can lead a very healthy, happy and productive life. Much research, since our efforts in the mid 1990s is now designed to improve the health and cognitive abilities of people with Down syndrome.
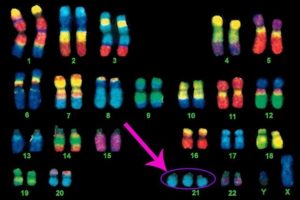
Nondysjunction Down syndrome karotype
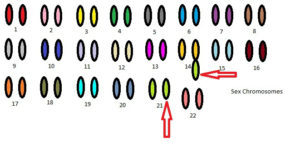
Translocation Down syndrome karotype
MTHFR MUTATIONS AND DOWN SYNDROME PREGNANCIES